Contrast-enhanced C-arm CT evaluation of radiofrequency ablation lesions in the left ventricle.
Girard EE, Al-Ahmad A, Rosenberg J, Luong R, Moore T, Lauritsch G, Boese J, Fahrig R.
Department of Bioengineering, Stanford University, Palo Alto, California 94304, USA.
OBJECTIVES: The purpose of this study was to evaluate use of cardiac C-arm computed tomography (CT) in the assessment of the dimensions and temporal characteristics of radiofrequency ablation (RFA) lesions. This imaging modality uses a standard C-arm fluoroscopy system rotating around the patient, providing CT-like images during the RFA procedure.
BACKGROUND: Both cardiac magnetic resonance (CMR) and CT can be used to assess myocardial necrotic tissue. Several studies have reported visualizing cardiac RFA lesions with CMR; however, obtaining CMR images during interventional procedures is not common practice. Direct visualization of RFA lesions using C-arm CT during the procedure may improve outcomes and circumvent complications associated with cardiac ablation procedures.
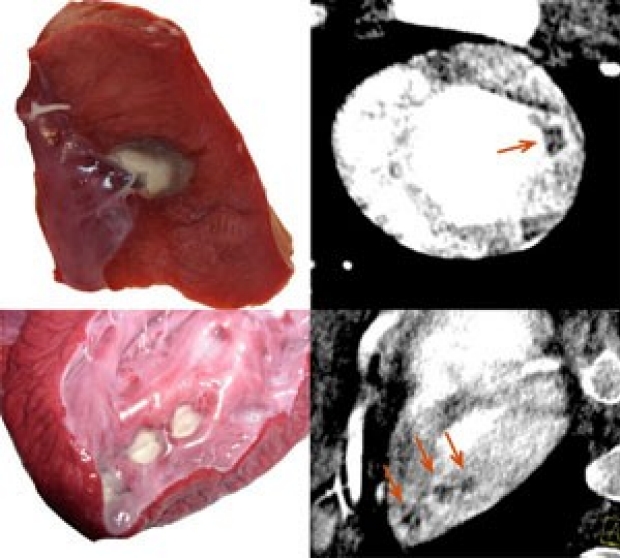
METHODS: RFA lesions were created on the endocardial surface of the left ventricle of 9 swine using a 7-F RFA catheter. An electrocardiographically gated C-arm CT imaging protocol was used to acquire projection images during iodine contrast injection and after the injection every 5 min for up to 30 min, with no additional contrast. Reconstructed images were analyzed offline. The mean and SD of the signal intensity of the lesion and normal myocardium were measured in all images in each time series. Lesion dimensions and area were measured and compared in pathologic specimens and C-arm CT images.
RESULTS: All ablation lesions (n = 29) were visualized and lesion dimensions, as measured on C-arm CT, correlated well with postmortem tissue measurements (linear dimensions: concordance correlation = 0.87; area: concordance correlation = 0.90. Lesions were visualized as a perfusion defect on first-pass C-arm CT images with a signal intensity of 95 HU lower than that of normal myocardium (95% confidence interval: -111 HU to -79 HU). Images acquired at 1 and 5 min exhibited an enhancing ring surrounding the perfusion defect in 24 lesions (83%).
CONCLUSIONS: RFA lesion size, including transmurality, can be assessed using electrocardiographically gated cardiac C-arm CT in the interventional suite. Visualization of RFA lesions using cardiac C-arm CT may facilitate the assessment of adequate lesion delivery and provide valuable feedback during cardiac ablation procedures.
Towards cardiac C-arm computed tomography.
Lauritsch G, Boese J, Wigstrˆm L, Kemeth H, Fahrig R.
Siemens AG, Medical Solutions, 91301 Forchheim, Germany.
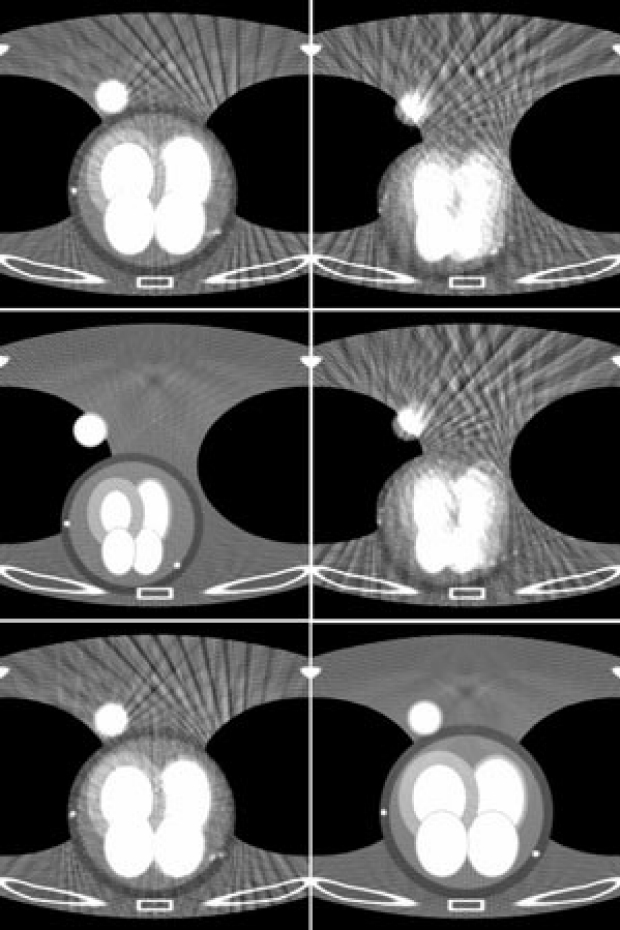
Cardiac interventional procedures would benefit tremendously from sophisticated three-dimensional image guidance. Such procedures are typically performed with C-arm angiography systems, and tomographic imaging is currently available only by using preprocedural computed tomography (CT) or magnetic resonance imaging (MRI) scans. Recent developments in C-arm CT (Angiographic CT) allow three-dimensional (3-D) imaging of low contrast details with angiography imaging systems for noncardiac applications. We propose a new approach for cardiac imaging that takes advantage of this improved contrast resolution and is based on intravenous contrast injection. The method is an analogue to multisegment reconstruction in cardiac CT adapted to the much slower rotational speed of C-arm CT. Motion of the heart is considered in the reconstruction process by retrospective electrocardiogram (ECG)-gating, using only projections acquired at a similar heart phase. A series of N almost identical rotational acquisitions is performed at different heart phases to obtain a complete data set at a minimum temporal resolution of 1/N of the heart cycle time. First results in simulation, using an experimental phantom, and in preclinical in vivo studies showed that excellent image quality can be achieved.
Cardiac C-arm CT: a unified framework for motion estimation and dynamic CT.

Pruemmer M, Hornegger J, Lauritsch G, Wigstrˆm L, Girard-Hughes E, Fahrig R.
Chair of Pattern Recognition, FA-University Erlangen-Nuremberg, 91054 Nuremberg, Germany.
Generating 3-D images of the heart during interventional procedures is a significant challenge. In addition to real time fluoroscopy, angiographic C-arm systems can also now be used to generate 3-D/4-D CT images on the same system. One protocol for cardiac CT uses ECG triggered multisweep scans. A 3-D volume of the heart at a particular cardiac phase is then reconstructed by applying Feldkamp (FDK) reconstruction to the projection images with retrospective ECG gating. In this work we introduce a unified framework for heart motion estimation and dynamic cone-beam reconstruction using motion corrections. The benefits of motion correction are 1) increased temporal and spatial resolution by removing cardiac motion which may still exist in the ECG gated data sets and 2) increased signal-to-noise ratio (SNR) by using more projection data than is used in standard ECG gated methods. Three signal-enhanced reconstruction methods are introduced that make use of all of the acquired projection data to generate a 3-D reconstruction of the desired cardiac phase. The first averages all motion corrected back-projections; the second and third perform a weighted averaging according to 1) intensity variations and 2) temporal distance relative to a time resolved and motion corrected reference FDK reconstruction. In a comparison study seven methods are compared: nongated FDK, ECG-gated FDK, ECG-gated, and motion corrected FDK, the three signal-enhanced approaches, and temporally aligned and averaged ECG-gated FDK reconstructions. The quality measures used for comparison are spatial resolution and SNR. Evaluation is performed using phantom data and animal models. We show that data driven and subject-specific motion estimation combined with motion correction can decrease motion-related blurring substantially. Furthermore, SNR can be increased by up to 70% while maintaining spatial resolution at the same level as is provided by the ECG-gated FDK. The presented framework provides excellent image quality for cardiac C-arm CT.